DCS Technique (continued)
SPECIAL TECHNIQUES
Using the DCS for Subtrochanteric Fractures
Indications
The DCS is indicated for the following fractures of the
proximal femur:
- Transverse subtrochanteric fractures *
- Short oblique subtrochanteric fractures *
- Long oblique subtrochanteric fractures *
* With the lesser trochanter avulsed or on the distal
fragment (femoral shaft) (2).
The design of the DCS Plate can enhance fixation of
selected, stable subtrochanteric fractures because it permits
stable fixation in the proximal fragment (3). The DCS Plate has
a 95° barrel angle, allowing it to enter the femur more prox-
imally than the DHS Plate and allowing insertion of two or
more screws into the calcar. Further, its two round proximal
plate holes permit insertion of 6.5 mm Cancellous Bone
Screws, for stable proximal fixation.
- Stable transverse and short oblique subtrochanteric fractures.
When using the DCS Plate for these fractures, the plate
can act as a tension band against normal medial com-
pressive forces (4).
- Long oblique subtrochanteric fractures.
When using the
135° DHS Plate to treat long oblique subtrochanteric frac-
tures, use of the proximal plate screws can prohibit com-
pression. With the 95° DCS Plate, however, stable fixation
can be achieved by lagging the fracture through the plate,
since controlled collapse is not anticipated.
Note: When used in the proximal femur, the DCS Plate can
only be used to treat stable fractures; i.e., fractures that can
be directly reduced and anatomically reassembled to allow
restoration of the bony medial buttress. Because the DCS
Plate has a 95° barrel angle, it does not allow for controlled
collapse and compression.
Preoperative Considerations
- Insertion of the DHS/DCS Guide Pin
Though the general insertion area of the guide pin
is known, the precise insertion point varies with the CCD
angle, or the angle subtended between the femoral neck and
shaft axes. Assessment of the CCD angle will allow subse-
quent placement of the lag screw in its optimal position-in
the center of the femoral neck and in the inferior half of the
femoral head. (See illustration below) This insertion point should
be determined preoperatively with the aid of planning
templates.
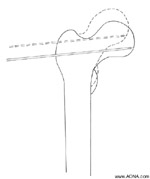
Click for enlarged view of image
The insertion point of the guide pin will vary with CCD angle (angle
subtended between the femoral neck and shaft axes), as depicted by
this valgus femur (dotted lines). Example is exaggerated for clarity.
(2) Roy Sanders and P. Regazzoni, "Treatment of Subtrochanteric Femur
Fractures Using the Dynamic Condylar Screw" Journal of Orthopaedic Trauma
vol. 3, no. 3 (New York: Raven Press, 1989) 211.
Next Page
DHS / DCS Index